
IRS FORM 1095-B
Last modified by andrew k on 2026/03/18 23:38
FORM 1095-B
Click on the individual boxes below for specific IRS Instructions
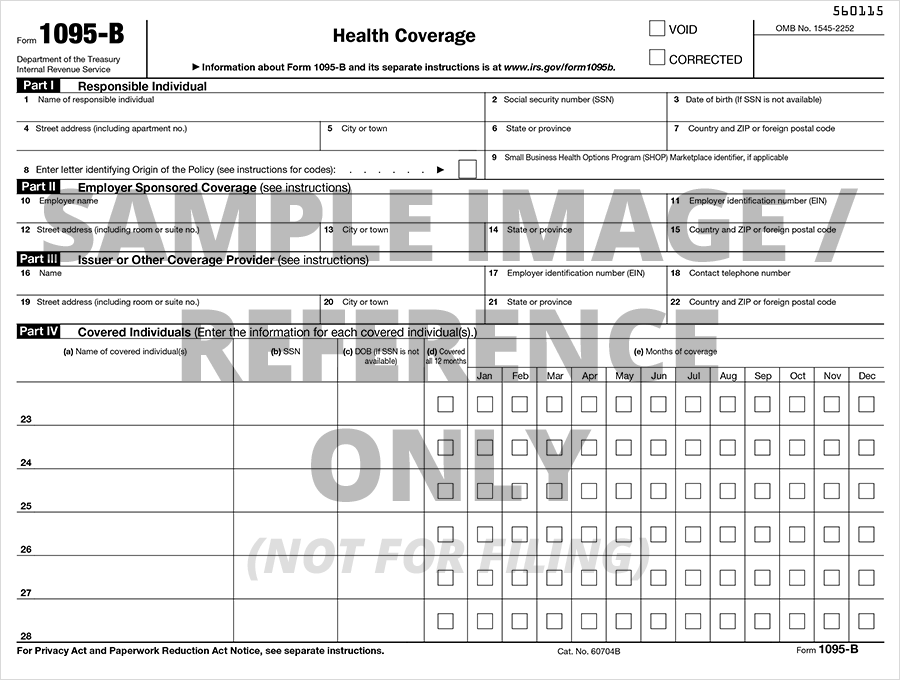
| Part II: Employer-Sponsored Coverage |
| Lines 10-15, Name, EIN, and Complete Mailing Address for the Employer Sponsoring the Coverage |
| Part III: Issuer or Other Coverage Provider |
| Lines 16-22, Name, EIN, and Complete Mailing Address of Issuer/ Other Coverage |
| Part IV: Covered Individuals |
| Column (a), Covered Individual's Name |
| Column (b), Covered Individual's Social Security Number (SSN) |
| Column (c), Covered Individual's Birthdate (MM/DD/YYY) if Social Security Number (SSN) is not available |
| Column (d), Covered all 12 months |
| Column (e), Months of Coverage |
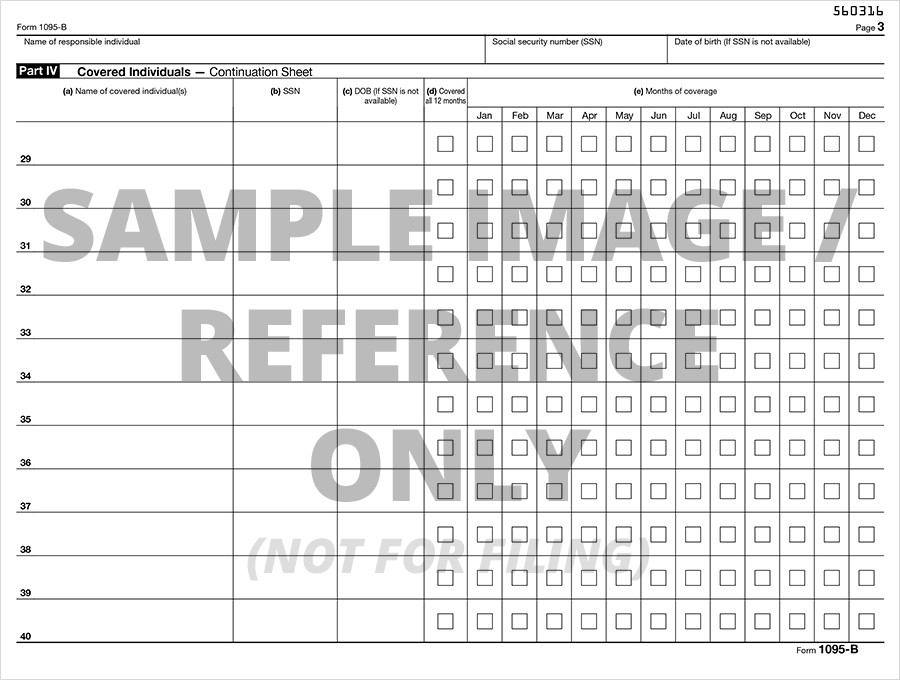
| Part IV: Covered Individuals (Continuation) |
| Column (a), Name of each Covered Individual |
| Column (b), Social Security Number (SSN) of each Covered Individual |
| Column (c), Birthdate (MM/DD/YYY) of each Covered Individual if SSN is not available |
| Column (d), Individual Covered for 12 months |
| Column (e), Coverage each month if individual wasn't covered for all 12 months |